Parents & Families
Finding out that your child has a diagnosis of Trisomy 18 is life-changing. You face an uncertain future and have many, many questions.
It is very likely that prior to learning of your child’s diagnosis, you were unfamiliar with Trisomy 18. While considered rare medically, Trisomy 18 is a life-threatening genetic disorder that impacts about 1 out of every 2000 pregnancies in the U.S. You and your child are not alone.
We have the resources and answers you need to understand your child’s diagnosis and make informed decisions about their health. We can also connect you with other families in our community who have faced these same challenges.
What is Trisomy 18?
Trisomy 18, also known as Edwards syndrome, is a condition that is caused by an error in cell division, known as meiotic disjunction. When this happens, instead of the normal pair, an extra chromosome 18 (a triple) results in the developing baby and disrupts the normal pattern of development in significant ways that can be life-threatening, even before birth. A Trisomy 18 error occurs in about 1 out of every 2000 pregnancies in the United States and 1 in 6000 live births. The number of total births is much higher because it includes significant numbers of stillbirths that occur in the 2nd and 3rd trimesters of pregnancy.
Unlike Down syndrome, or Trisomy 21, which also is caused by an extra chromosome, the developmental issues caused by Trisomy 18 are associated with medical complications that are more potentially life-threatening in the early months and years of life. Studies have shown that only 50% of babies who are carried to term will be born alive. At birth, intensive care admissions in Neonatal Intensive Care Units (NICU’s) are routine for infants with Trisomy 18.
At conception, 23 chromosomes from the father and 23 chromosomes from the mother combine to create a baby with a set of 46 chromosomes in each cell. A trisomy occurs when a baby has three #18 chromosomes instead of the normal two. This is something that happens at conception. And although many parents worry about this, it is important to know that parents have done nothing before or during pregnancy to cause this disorder in their child.
The most common trisomy is Trisomy 21, also known as Down syndrome, where a baby has three of the twenty-first chromosome. Trisomy 18 is the second most common trisomy and occurs when a baby has three of the eighteenth chromosome. This results in 47 chromosomes instead of the normal 46 in the affected cells. It is this extra genetic material that causes the developmental problems associated with Trisomy 18. The third most common is Trisomy 13, also known as Patau syndrome.
While there are different types of Trisomy 18, this does not mean one is better for a child than another. With each type, there is a range of possibilities. Some children are medically fragile while others thrive; some children walk while others are confined to wheelchairs. It is hard to say how the extra chromosome will impact an individual child from the genetic diagnosis alone.
Types of Trisomy 18:
- Full Trisomy 18: The most common type of Trisomy 18 (occurring in about 95% of all cases) is full Trisomy. With full Trisomy, the extra chromosome occurs in every cell in the baby's body. This type of trisomy is not hereditary. It is not due to anything the parents did or did not do—either before or during pregnancy.
- Partial Trisomy 18: Partial trisomies are very rare. They occur when only part of an extra chromosome is present. Some partial Trisomy 18 syndromes may be caused by hereditary factors. Very rarely, a piece of chromosome 18 becomes attached to another chromosome before or after conception. Affected people have two copies of chromosome 18, plus a "partial" piece of extra material from chromosome 18.
- Mosaic Trisomy 18: Mosaic trisomy is also very rare. It occurs when the extra chromosome is present in some (but not all) of the cells of the body. Like full Trisomy 18, mosaic Trisomy is not inherited and is a random occurrence that takes place during cell division.
The genetic material from the extra eighteenth chromosome can cause a variety of medical and developmental problems that occur with varying severity. Just as children with Down syndrome can range from mildly to severely affected, the same is true for children with Trisomy 18. This means that there is no hard and fast rule about what Trisomy 18 will mean for your child. However, statistics unfortunately show that there is a high mortality rate for children with Trisomy 18 before or shortly after birth.
Typical characteristics of Trisomy 18 include:
- Heart defects:
- VSD (Ventricular Septal Defect): a hole between the lower chambers
- ASD (Atrial Septal Defect): a hole between the upper chambers
- Coarctation of the aorta: a narrowing of the exit vessel from the heart
- Kidney problems
- Part of the intestinal tract outside of the stomach (omphalocele)
- The esophagus doesn’t connect to the stomach (esophageal artesia)
- Excess amniotic fluid (polyhydramnios)
- Clenched hands
- Pocket of fluid on the brain (choroid plexus cysts)
- Rocker bottom feet
- Delayed growth
- Small jaw (mycrognathia)
- Small head (microcephaly)
- Low-set ears
- Strawberry-shaped head
- Severe developmental delays
- Umbilical or inguinal hernia
The extra genetic material from the extra eighteenth chromosome can cause a wide variety of medical and developmental problems (sometimes referred to as birth defects) in the developing child in the mother’s womb and after birth. Just as children with Down syndrome can range from mildly to severely affected, the same is true for children with Trisomy 18.
This means that there is no hard and fast rule about what Trisomy 18 will mean for a specific child. Each child has their own unique profile of how Trisomy 18 is affecting their developing body and organs. However, all studies on survival rates show that there is a high mortality rate for children with Trisomy 18 before or shortly after birth.
How Is Trisomy 18 Diagnosed?
Most cases of Trisomy 18 are diagnosed prenatally in the United States. Regardless of whether the diagnosis is made prenatally or postnatally (after birth), the process is the same. A sample of the baby’s DNA is extracted from a blood sample or other bodily cells or tissue and is cultured to examine a picture of the chromosomes called a karyotype.
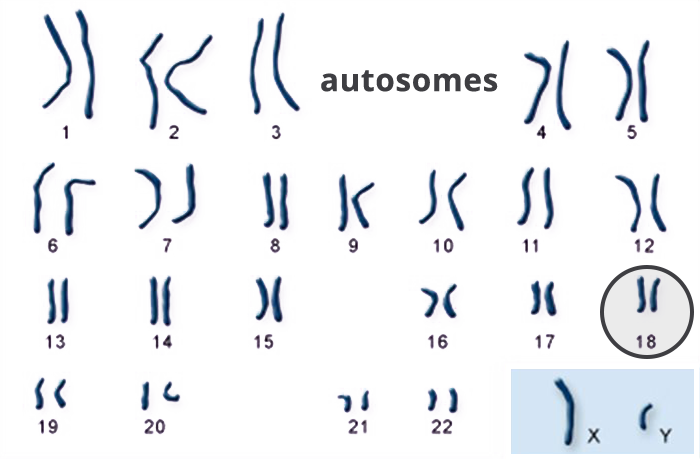
A karyotype is simply a picture of a person’s chromosomes. In order to get this picture, the chromosomes are isolated, stained, and examined under the microscope. Most often, this is done using the chromosomes in the white blood cells. A picture of the chromosomes is taken through the microscope. A visible extra 18th chromosome confirms a Trisomy 18 diagnosis.
A lot of prenatal testing is available which may indicate Trisomy 18. It is important to understand that there are two types of testing: screening and diagnostic.
These tests indicate a risk or likelihood that Trisomy 18 is present. These tests take the results of everyone who has had the same testing, and they compare your specific results with that group. Then they use statistics to identify the odds that it is present in your child, based upon the number of times others with the same test results have had children with Trisomy 18 in the past.
This is much the same way that weather is forecast, by saying there is a 20% chance of rain because 20% of the time when the conditions were the same, it has rained. Just as the weather forecast is not completely accurate, screening tests are not a diagnosis but only an indication that the risk is higher than normal.
The following are screening tests, which CANNOT diagnose Trisomy 18:
AFP (also known as triple screen, quad screen, maternal serum screening)
The quad screen — also known as the quadruple marker test, the second-trimester screen or simply the quad test — is a prenatal test that measures levels of four substances in pregnant women's blood:
- Alpha-fetoprotein (AFP), a protein made by the developing baby
- Human chorionic gonadotropin (HCG), a hormone made by the placenta
- Estriol, a hormone made by the placenta and the baby's liver
- Inhibin A, another hormone made by the placenta
Ideally, the quad screen is done between weeks 15 and 18 of pregnancy — during the second trimester. However, the procedure can be done up to week 22.
The quad screen is used to evaluate whether your pregnancy has an increased chance of being affected with certain conditions, such as Trisomy 18. If your risk is low, the quad screen can offer reassurance that there is a decreased chance for Trisomy 18 or other conditions.
If the quad screen indicates an increased chance of one of these conditions, you might consider diagnostic testing to determine whether your baby has Trisomy 18.
Ultrasound (standard, level II, level III, 3D)
Diagnostic ultrasound, also called sonography or diagnostic medical sonography, is an imaging method that uses high-frequency sound waves to produce images of structures within your body. Ultrasound is used during pregnancy to check the baby’s development, the presence of multiple pregnancies and to screen for conditions such as Trisomy 18.
If fetal abnormalities are detected, you may be offered further tests to confirm the diagnosis, such as amniocentesis and chorionic villus sampling.
These tests check actual cells and can determine if Trisomy 18 is actually present. This is a diagnosis since the condition has actually been found in the cells.
The following are diagnostic tests, which CAN diagnose Trisomy 18:
CVS (Chorionic Villi Sampling)
Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed from the placenta for testing. The sample can be taken through the cervix (transcervical) or the abdominal wall (transabdominal).
During pregnancy, the placenta provides oxygen and nutrients to the growing baby and removes waste products from the baby's blood. The chorionic villi are wispy projections of placental tissue that share the baby's genetic makeup. The test can be done as early as 10 weeks of pregnancy.
Chorionic villus sampling can reveal whether a baby has a chromosomal condition, such as Trisomy 18 or Down syndrome, as well as other genetic conditions, such as cystic fibrosis.
Amnio (Amniocentesis, FISH test)
Amniocentesis is a procedure used to take out a small sample of the amniotic fluid for testing. This is the fluid that surrounds the fetus in a pregnant woman. Amniotic fluid is a clear, pale yellow fluid that:
- Protects the fetus from injury
- Protects against infection
- Allows the baby to move and develop properly
- Helps control the temperature of the fetus
Along with various enzymes, proteins, hormones, and other substances, the amniotic fluid contains cells shed by the fetus. These cells have genetic information that can be used to diagnose genetic disorders, such as Trisomy 18, and open neural tube defects (ONTDs), such as spina bifida.
The fluid is sent to a lab so that the cells can grow and be analyzed. Results are most often ready in about 10 days to 14 days, depending on the lab.
Knowing which test was used is important in deciding what your next steps are. If a screening test has resulted in an elevated risk of Trisomy 18, a diagnostic test can be performed to determine whether your child has Trisomy 18. If a diagnostic test indicates a Trisomy 18 diagnosis, you will be faced with making decisions about your child’s care.